Youth's Lives Every Day
Key Findings
- TGNB young people of color who had high levels of family support had a 34% lower odds of attempting suicide in the past year than those with low to moderate levels of family support.
- Having high levels of social support from friends and living in an accepting community were both associated with a 28% lower odds of considering suicide in the past year.
- TGNB young people of color are not monolithic; race/ethnicity was related to health care access, mental health, and suicide.
Background
Transgender and nonbinary (TGNB) young people of color exist at a nexus of vulnerabilities by virtue of how society treats them. True to the intersectional nature of their lived experiences,1 TGNB people of color are frequently subjected to harmful social determinants of health such as discrimination, limited economic opportunity, and barriers to accessing health care, often resulting in poor mental and physical health outcomes.2
Despite myriad challenges, TGNB young people of color not only survive—they thrive. A crucial factor that is often cited in their resilience is the availability of social support.3 This support is broadly defined as both the perception and the reality of receiving help from others, as well as feeling connected to a supportive network.4 There are different ways to provide social support, and this often depends on the relationship between individuals (e.g., a person receives different types of support from their friends than their parents). However, due to varying contexts related to factors including culture, economic constraints, and the policy environment, the circumstances under which people receive social support change for people of color and LGBTQ+ people.5,6 Despite this knowledge, little is known about how social support functions in the lives of TGNB young people of color, namely from whom they receive it and its effect on their health. Using data from The Trevor Project’s 2024 U.S. National Survey on the Mental Health of LGBTQ+ Young People, this brief examines the role of social support from: 1) friends, 2) family, and 3) community acceptance on health care access, mental health, and suicide among TGNB young people of color ages 13 to 24.
Results
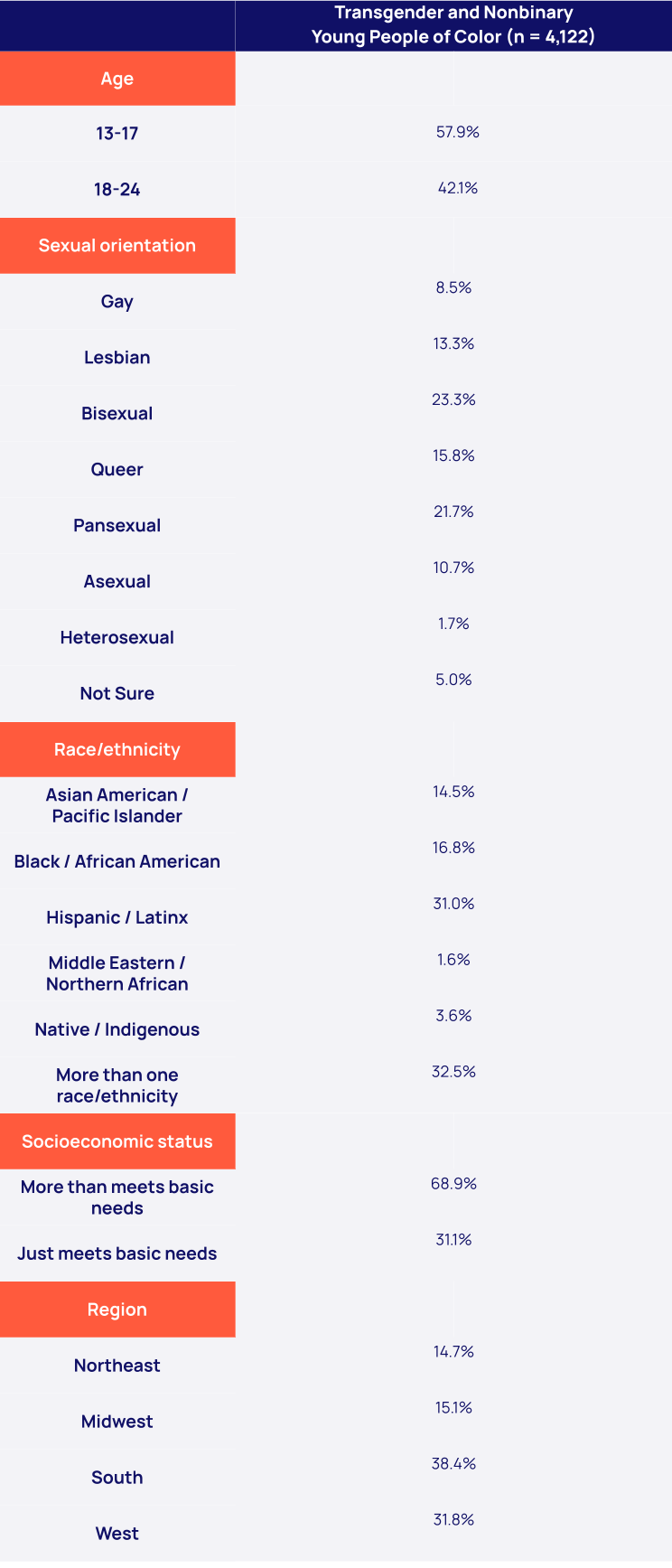
TGNB young people of color (n = 4,122) experienced varying levels of access to health care, mental health outcomes, and suicidal thoughts and behaviors. In terms of health care, only 47% of those who desired mental health care in the past year said they were able to access it. Among the 73% who reported wanting access to at least one form of transgender health care, only 17% were able to access it. A majority (70%) reported experiencing recent symptoms of anxiety, and 61% reported recent symptoms of depression. Nearly half (48%) of TGNB young people of color considered suicide in the past year, and 16% attempted suicide in the past year.
Social support
TGNB young people of color reported receiving social support in different ways: 67% reported high levels of support from friends, 17% from family, and 65% said they lived in an accepting community. While there were no racial differences in receiving social support from friends, there were notable differences in family support and perceptions of community acceptance. For example, Black TGNB young people and Middle Eastern and Northern African TGNB young people were the least likely to report high levels of family social support, while Native and Indigenous TGNB young people were the least likely to report living in an accepting community. Though there were differences in who received social support, its effect was consistent: those who received high levels of social support had greater access to desired health care and lower rates of anxiety, depression, suicidal ideation, and suicide attempts.

Access to health care
TGNB young people of color with high family support had over twice the odds of receiving desired mental health care than those with low or moderate levels of family support (aOR = 2.62 95% CI = 2.10 – 3.28, p<.001). There were racial differences with access as well, with Black (aOR = 0.67, 95% CI = 0.52 – 0.86, p<.01) and Latinx (aOR = 0.81, 95% CI = 0.66 – 0.99, p<.05) TGNB young people being less likely to access desired mental health care than their multiracial peers.
Sexual orientation was associated with receiving desired transgender health care. Pansexual (aOR = 0.60, 95% CI = 0.41 – 0.81, p<.01) and asexual (aOR = 0.54, 95% CI = 0.34 – 0.86, p<.01) TGNB of color were less likely to receive this care compared to bisexual TGNB young people of color. Heterosexual (aOR = 5.67, 95% CI = 2.71 – 11.95, p<.001) and gay (aOR = 1.66, 95% CI = 1.07 – 2.58, p<.05) TGNB young people of color, however, were more likely to have received care than their bisexual peers. Region was also associated with receipt of desired transgender health care. Compared to those living in the South, TGNB young people of color in the Northeast (aOR = 1.84, 95% CI = 1.26 – 2.69, p<.01), Midwest (aOR = 1.72, 95% CI = 1.19 – 2.49, p<.01), and West (aOR = 1.48, 95% CI = 1.08 – 2.03, p<.05) were more likely to receive desired transgender health care. Support from friends and community acceptance was not associated with receiving desired care, although compared to those with low to moderate family support, TGNB young people of color with high family support had over twice the odds of receiving desired transgender health care (aOR = 2.53, 95% CI = 1.90 – 3.37, p<.001).
Mental health
High levels of family social support (aOR = 0.81, 95% CI = 0.66 – 0.99, p<.05) and community acceptance (aOR = 0.70, 95% CI = 0.58 – 0.85, p<.001) were both associated with a lower likelihood of recent anxiety symptoms compared to those who had low to moderate levels of family support and community acceptance, respectively. There were racial differences as well, with Asian American and Pacific Islander (aOR = 0.64, 95% CI = 0.50 – 0.83, p<.001), Black (aOR = 0.63, 95% CI = 0.49 – 0.82, p<.001), and Hispanic and Latinx (aOR = 0.75, 95% CI = 0.61 – 0.92, p<.01) TGNB young people less likely to report recent anxiety symptoms than their multiracial peers.
Having high levels of support from each of the three examined sources was associated with a lower likelihood of depression: friends (aOR = 0.71, 95% CI = 0.60 – 0.84, p<.001), family (aOR = 0.54, 95% CI = 0.45 – 0.66, p<.001), and community acceptance (aOR = 0.66, 95% CI = 0.55 – 0.79, p<.001). Asian American and Pacific Islander (aOR = 0.70, 95% CI = 0.55 – 0.90, p<.001) TGNB young people were less likely to report recent depression than their multiracial peers.

Suicide
TGNB young people of color who had high levels of support from friends (aOR = 0.72, 95% CI = 0.60 – 0.85, p<.001), family (aOR = 0.68, 95% CI = 0.55 – 0.84, p<.001), and community acceptance (aOR = 0.72, 95% CI = 0.61 – 0.87, p<.001) were all less likely to have considered suicide in the past year compared to those with low to moderate levels of support from each of these sources.
There were also differences by sexual orientation. Pansexual TGNB young people of color were more likely to have attempted suicide in the last year compared to their bisexual peers (aOR = 1.72, 95% CI = 1.19 – 2.49, p<.01), and asexual TGNB young people of color were less likely (aOR = 0.60, 95% CI = 0.38 – 0.96, p<.05). Asian American and Pacific Islander (aOR = 0.66, 95% CI = 0.45 – 0.96, p<.05) TGNB young people were less likely to attempt suicide in the past year compared to their multiracial peers. Native and Indigenous TGNB young people, however, had twice the odds (aOR = 2.02, 95% CI = 1.19 – 2.49, p<.01) of a suicide attempt in the past year. Having high family support was associated with 34% lower odds of a suicide attempt in the past year (aOR = 0.66, 95% CI = 0.48 – 0.91, p=.01).
Looking Ahead
TGNB young people of color face a unique set of challenges; however, these findings highlight that having access to social support from friends, family, and community can significantly enhance their overall health and well-being. Though much of the existing research has documented the benefits of social support among people of color and LGBTQ+ adults separately, much less has looked at those who exist at the intersection, particularly young people.
While social support broadly was associated with better outcomes in our analysis, the source of that support mattered. High levels of social support from friends was strongly associated with lower rates of depression and suicidal ideation. However, high support from friends did not correlate with receipt of desired mental or transgender health care—likely due to the fact that the types of support TGNB young people of color receive from friends are not aligned with overcoming the barriers necessary to access either type of care. Similarly, living in a supportive community was also associated with lower rates of anxiety, depression, and suicidal ideation, but did not translate into improved access to desired health care. Our finding that the region of the country where a TGNB young person lives was associated with receiving transgender health care is consistent with the fact that many barriers to this care are determined by state-level policy rather than community support alone.7
The most robust finding in this analysis centers on family support. Having high levels of family support was the one factor consistently associated with improved access to health care, lower rates of anxiety and depression, and a lower likelihood of considering and attempting suicide. For young people, families are often the primary source of tangible instrumental support such as housing, health care, and other basic needs, all of which are all highly correlated with health.8 Importantly, even after controlling for socioeconomic status in our models, high family support still had the strongest effect among the examined sources of support. This suggests that family support reflects more than just access to resources—it captures a fundamental experience related to the ability of TGNB young people to be safe, comfortable, and affirmed in their own homes.
This analysis also provided a rare opportunity to explore racial differences beyond aggregating all non-White participants. This is particularly challenging to do in research with LGBTQ+ populations given the limitations of sample sizes, but we hope these findings underscore the importance of doing so whenever possible. Nevertheless, our findings with respect to race/ethnicity are better articulated as a starting point rather than a conclusion. For example, though Native and Indigenous TGNB young people were the least likely to report living in an accepting community (47%), they were also the most likely to have received high family support (24%). Though this analysis alone cannot provide reasons why, it does suggest that any intervention aimed at working with Native and Indigenous families and communities must recognize and sufficiently incorporate these unique dynamics in order to be effective. And while rates for high family support were relatively low for all TGNB young people in this analysis, as little as 10% of both Black and Middle Eastern and Northern African respondents said they received it. Yet it is likely the vast majority of those families don’t perceive the support they provide as being inadequate. By talking more with families, especially the parents and caregivers of TGNB young people, we can better equip families to provide the social support they want and that their child needs.
While TGNB young people of color still face incredibly potent structural challenges, these findings suggest that with the support of friends, family, and community, many of these effects can be ameliorated. Providing social support to TGNB young people of color is a public health intervention.
The Trevor Project is committed to supporting LGBTQ+ young people through crisis intervention, research, and advocacy initiatives. Our 24/7 crisis services—available by phone, chat, and text—ensure that LGBTQ+ youth can connect with trained counselors whenever they need support, regardless of their mental health diagnosis or presentation. In response to the high rates of comorbid mental health conditions and widespread desire for care—including among youth without formal diagnoses—our services are designed to meet young people where they are in their mental health journey. TrevorSpace, our dedicated social networking platform, provides a safe and welcoming space for LGBTQ+ young people to connect with supportive peers, helping to reduce isolation and promote community support. Our education team equips adults with the tools needed to support LGBTQ+ youth across diverse identities and experiences, including those navigating multiple diagnoses, systemic barriers, and unmet care needs. Meanwhile, our advocacy team works at the local, state, and federal level to promote access to inclusive, supportive environments and affirming mental health care. We remain committed to publishing research that explores the nuanced mental health experiences of LGBTQ+ youth, especially those impacted by structural inequities, to drive informed policy and life-saving intervention.
You can read more related research from The Trevor Project here: How to Best Support Transgender and Nonbinary Young People, The Mental Health and Well-Being of Indigenous LGBTQ Young People, The Role of Parent and Caregiver Support on Perceived Life Expectancy and Life Purpose for Black Transgender and Nonbinary Young People, The Mental Health and Well-Being of Latinx LGBTQ Young People, Middle Eastern and Northern African LGBTQ+ Young People, and The Mental Health and Well-Being of Asian American and Pacific Islander (AAPI) LGBTQ Youth. Additionally, The Trevor Project provides resources for both LGBTQ+ young people and their allies, such as Friends & Family Support Systems for LGBTQ+ Youth and Black & LGBTQ+: Approaching Intersectional Conversations.
Data Tables
Characteristics of Transgender and Nonbinary Youth of Color 2024 U.S. National Survey Respondents
Methods
References
Recommended Citation
The Trevor Project (2025). Friends, Family, and Community: Social Support and the Health of Transgender and Nonbinary Young People of Color. https://doi.org/10.70226/WKQJ1410
For more information please contact: [email protected]
© The Trevor Project 2025